I am a member of a hair related WhatsApp group of mostly doctors and surgeons. Various physicians in there sometimes post close-up images of patient scalps. Perhaps the most common photo and imaging technology that is utilized is TrichoScan® (Germany).
Surprisingly, the TrichoScan company website does not have SSL and the homepage has a last update from 2018. The same applies when it comes to the related Tricholog website.
Another German company whose name I have sometimes seen used in tandem with TrichoScan is Fotofinder and its Trichoscale DX. Their automated digital hair analysis technology seems quite impressive. They also offer trichoscopy hair consultations via their TrichoLAB service. Perhaps all of these German companies are related to each other and there is some rebranding going on.
TrichoScan Digital Image Hair Growth Analysis
According to a 2003 article by Rolf Hoffman (associated with the manufacturer) on the at-the-time novel TrichoScan tool:
“TrichoScan as a method that combines epiluminescence microscopy with automatic digital image analysis for the measurement of human, and potentially animal hair, in situ.”
More importantly, TrichoScan is able to analyze all four of the key biologic parameters of hair growth:
- Hair density (number per cm2).
- Hair diameter (μm).
- Hair growth rate (mm per day).
- The anagen/telogen ratio (see hair growth cycle).
In 2010, Dr. Rachita Dhurat and Dr. Punit Saraogi of India found some issues with the accuracy of TrichoScan. In particular, they found that anagen/telogen hair detection is not optimal; total hair density is overestimated; and the vellus hair percentage does not correlate with alopecia severity.
The manufacturer responded in detail to these accusations and also admitted that the very dark Asian hair color can cause some issues in readings. However, these can be resolved with a slight adjustment of the TrichoScan settings. Moreover, the device is now in its third generation and has been significantly refined over the years.
In 2022, a study from China found that TrichoScan was a very useful imaging tool in estimating the exact level of Ludwig hair loss classification in females. This was based on hair density and terminal hair percentage measurements in the midscap region via trichoscopic pictures.
TrichoScan Before and After Images
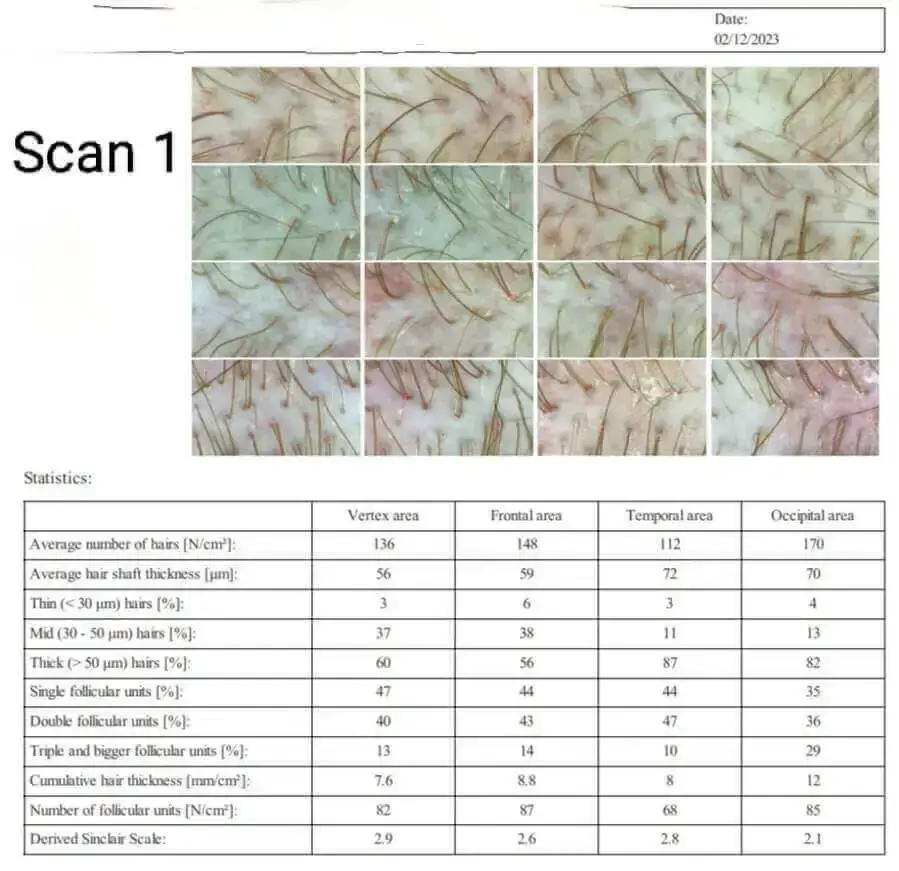
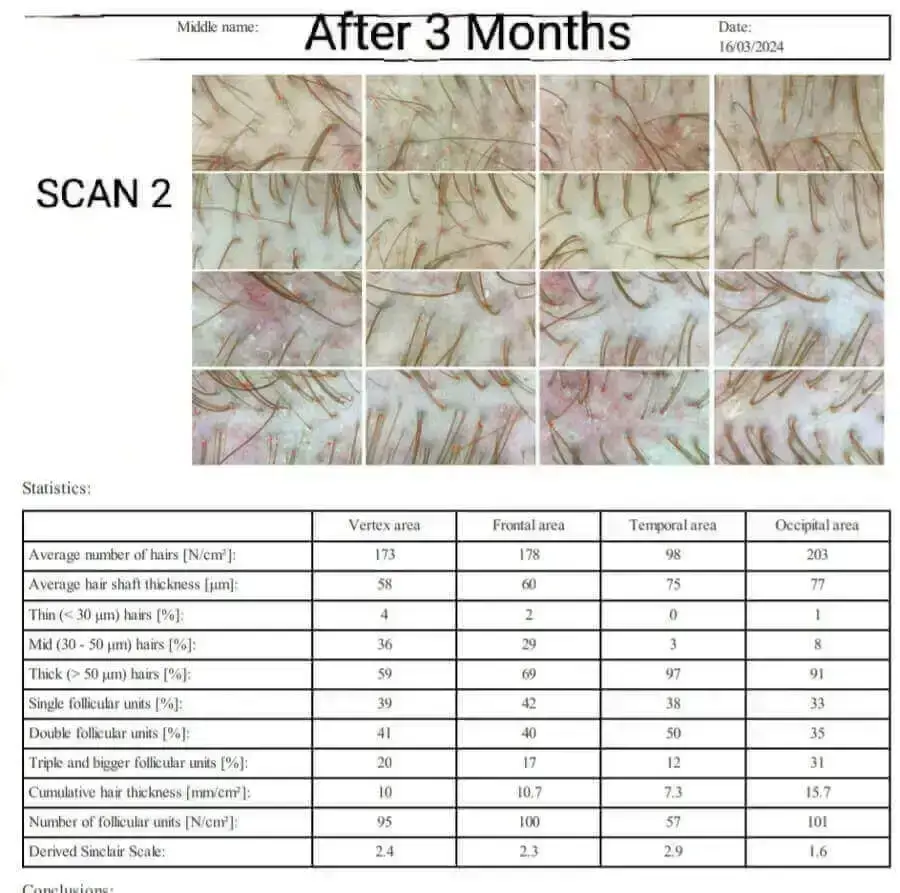
A few days ago, a Niostem device user named “Falcon” sent me some very interesting before and after 3-month photos of his TrichoScan hair growth analysis. He intends to update us again at the 6-month mark. He got his readings via TrichoLAB, which I mentioned earlier. He has posted many helpful comments on this site, and also on Reddit. Note that Niostem and TrichoLAB are both based in Germany.
I do not want to pay too much attention to just one data point, but “Falcon” does seem reliable. Moreover, his overall positive (+20%) hair growth increase data also shows a decrease in one (temporal) region of the scalp. This adds to his trustworthiness in my opinion. Personally, I am skeptical that Niostem can cause hair growth in totally bald regions of the scalp. However, thickening of existing hair and reversal of recent hair loss via electric stimulation has been proven in some studies.
TricoPat
While I have discussed a number of “Tricho” prefixed scalp hair image analysis brands and companies in this post, TricoPat is entirely different. I am only mentioning this company here because it is also sometimes brought up in our WhatsApp group. According to the Italy and Poland based company’s website:
“TRICOGENESI® is a patented treatment protocol developed by the association of TRICOPAT® and growth factors vehiculated with iontophoresis.”
Somewhat interesting. Electrically-assisted transdermal drug delivery (iontophoresis) has been used for well over a century. It is also one of the techniques that can be used as a topical finasteride delivery system. In the TricoPat protocol, the serum that is applied contains 6 synthetic growth factors.
On a related note, check out the fairly new and popular Alma TED transepidermal delivery system for hair growth (via the use of ultrasound).
TrichoScan results for topical Minoxidil 5% use in men with AGA:
https://www.jaad.org/article/S0190-9622(03)03703-4/fulltext
Hey Admin, do you have any potential news on GT20029? I heard that the results should be out right around this quarter.
No, but worth checking Kintor’s news page regularly:
https://en.kintor.com.cn/news/3/
Many trichologists offer their patients a Trichotest to determine what will be the best treatment for their alopecia. Androgenetic alopecia is determined by several genes, the genes manifest their action through RNA and are transformed into proteins. Hormones are proteins and perhaps the most important in androgenetic alopecia is testosterone, although there are others such as cortisol (in stress), progesterone (in pregnant women)… That is why there are multiple ways to create new medications. Although it is true that there are several treatment options, the medication that is almost always effective in men is finasteride or dutasteride, because it acts by inhibiting the transformation of testosterone into dihydrotestosterone, which is the main hormone responsible for hair loss (in addition to others such as prostate enlargement or beard growth). And why, if DHT is present in all men, does baldness only manifest in people with a genetic history of baldness? Well, this is because androgen receptors appear in the hair follicles of people with androgenetic alopecia, which in turn are also proteins, determined by other genes to which DHT binds.
My question is: Couldn’t a trichogenic analysis method be possible to see which hairs have androgen receptors for DHT? Simply comparing the donor area of a person with alopecia with the hair from the affected area, the differences would be observed, right? If a person in whom part of their hairs in the donor area have been miniaturized, it would be possible to see the reason for the miniaturization since there are probably androgen receptors in their donor area and in future treatments it is important to determine through a trichogenic analysis that Hairs from the donor area do not have androgen receptors…
If testosterone to DHT is the issue, What I don’t get is surely u should bald earlier in life literally at 21 when ur testosterone levels r through the roof, compared to 41 when they are significantly lower?
Mutruk…the best way to think about androgenic alopecia is that of an interplay between genetics, hormones and time. The hair cycle takes years to fully collapse, if you’re lucky that is. Some scientists (Norman Orentreich for example) have long suggested that the proper term is actually androchronogenic alopecia, thus reflecting the role of the 3 drivers.
thanks John, agreed, it’s multiple factors and I guess after genetics it’s ultimately aging- your body can’t cope with the same environment the same way at 40, as it did when it was 20
Guess the same stands true for many body functions, it’s subject to the same environmental factors but just can’t manage them the same as u age..sadly