Update: September 8, 2025
IGF-1 Mimetic for Hair Regrowth
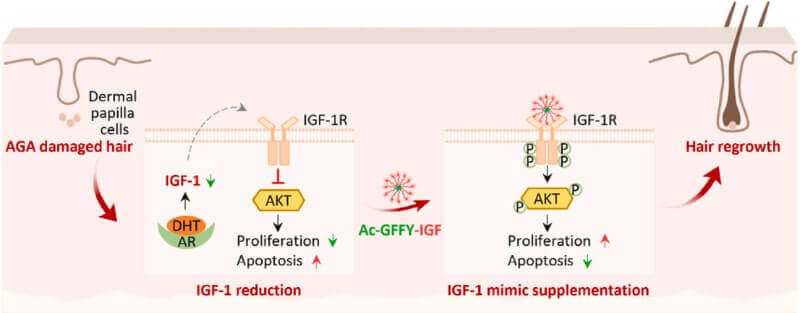
A new August 2025 study from China in relation to insulin-like growth factor 1 (IGF-1) and hair growth is making some waves in the hair loss world. The authors synthesized a biomimetic peptide of IGF-1 (called Ac-GFFY-IGF) that structurally and functionally mimicked IGF-1. Also of note, another recent Chinese study from July 2025 covered targeting IGF-1 induced cellular senescence in order to rejuvenate hair follicle aging.
In mouse models, it ended up:
- Promoting the proliferation of dermal papilla cells.
- Resisting dihydrotestosterone (DHT)-induced hair follicle apoptosis.
- Facilitating the transition of hair follicles from telogen (resting) to anagen (growing) phase.
- Promoting hair regrowth more effectively than minoxidil and native IGF-1 in androgenetic alopecia mouse models.
A Spain based dermatologist has covered this development in a detailed video:

March 30, 2015
IGF-1 and Hair Growth
In late 2014, I wrote about Shiseido’s Adenovital product made with Adenosine. The solid science behind this product, its popularity in Asia, and the good reputation of Shiseido all convinced me to add this product to the very short list of recommended hair loss products page on this site.
One of the studies in that blog post suggested that Adenosine promotes the expression of several growth factors responsible for hair growth, including fibroblast growth factors FGF-7 and FGF-2, insulin-like growth factor 1 (IGF-1), and vascular endothelial growth factor (VEGF).
I was planning to focus more on writing about these growth factors in 2015, and lo and behold I got my first chance several weeks ago when a new company called Follicept announced that it had developed a gel product that would deliver IGF-1 to the scalp and in the process bolster hair growth.
I was highly skeptical about this company at the time and remain so. Even after the Bald Truth Talk forum thread on this subject took off. It has some interesting posts from one of the company’s reps under the username “Follicept” whose real name is “Devon”.
Update: September 21, 2015 — In very sad news, Devon passed away at the very young age of 27.
For one, I am generally not a believer in new companies that are suddenly promoted enthusiastically in newspapers such as businesswire and are looking for funding. Moreover, this company had not even started testing on humans at the time of the initial publicity, although they were planning to do so very soon thereafter.
Also, while Follicept has some excellent material related to IGF-1 on their website, I was also not impressed by the grammar and appearance of parts of their site. But perhaps I am being too picky here and should just be glad that there are more companies working on baldness treatments.
In any case, Follicept does have some things going for it. For one, the company is connected to The University of Florida and Prometheon Pharma. The company’s CEO seems very intelligent and accomplished. The Follicept product is also going to be very low-cost (comparable to the price of Rogaine).
Most importantly, it seems like the company will not have to go through lengthy clinical trials, since IGF-1 has been used in humans for a while. In fact their are numerous studies supporting IGF-1’s beneficial properties when it comes to hair growth. So the product will quite likely be released by the end of this year as planned by the company assuming they get the funding they need. If effective, Follicept will also work for women.
One concern is that Shiseido’s Adenovital, while a very good product, never resulted in any kind of miracle result despite promoting the IGF-1 growth factor. Will Follicept be any better due to a possibly superior delivery mechanism? Can a new company that is still looking for funding produce something superior to a major established player such as Shiseido? I am not a believer, but it seems like quite a few people on the forums and on the chat on this site have an opposing viewpoint.

